.png)
Tactical Fitness: Navigating Injury Challenges
- ExultX
- Jun 6, 2024
- 17 min read
Updated: Jan 23

Topics Covered
1. Types of Injuries: Acute and Overuse
2. Injury Risk
3. Mitigating risk and enhancing injury resilience
4. Injury prevention models and rehabilitation
Summary
In this comprehensive exploration, we unravel the intricate tapestry of tactical fitness from the perspective of injury prevention and mitigation strategies that underpin the safety and effectiveness of our operators. By dissecting the nuances of injury types and unveiling the interplay of intrinsic and extrinsic risk factors, we uncover the pivotal role of evidence-based interventions in fortifying tactical resilience. As we delve into this article, we also explore the trenches of rehabilitation and return-to-duty models, where interdisciplinary collaboration and cutting-edge methodologies converge to forge a path towards enduring resilience in the face of adversity.
Discussing injury prevention and mitigation in tactical environments often involves navigating complexity and emotional intensity, influenced by deeply held beliefs and superstitions. Our aim in this article is to eliminate biases and provide clarity on this intricate topic. The reality is that injuries result from a complex interaction of multiple risk factors and only a fraction of which have been identified (1). Taken care, this publication does not claim to offer a universal solution to all the injuries, instead aims to provide a comprehensive exploration of injuries in tactical populations, focusing on their types, risk factors, prevention models, and rehabilitation and return to duty models. By examining the unique challenges faced by tactical populations and understanding the factors contributing to injuries, we can develop evidence-based recommendations to mitigate the risk of harm.
The significance of addressing injuries in tactical environments extends beyond the well-being of individual personnel. Injuries not only compromise the health and readiness of the affected operator but can also impact the overall effectiveness of the team or unit. A single injury can lead to a temporary loss of manpower, potentially affecting mission success and the safety of both the operator and their colleagues. Moreover, untreated, or mismanaged injuries can contribute to long-term health issues, impacting the during and post-service quality of life. Recognizing the importance of injury prevention and effective rehabilitation is, therefore, a fundamental aspect of optimizing the performance and longevity of tactical professionals (2–4).
1. Types of Injuries: Acute and Overuse
Due to the existence of various definitions, we need to provide clarification on what we define as injury:
Injury refers to tissue damage or other derangement of typical physical function in the body caused by engagement in sports, exercise, or occupational tasks. This harm typically arises from the rapid or repetitive kinetic energy transfer (5).
These injuries can be classified into two major categories: acute injuries and overuse injuries. Although we can delve into the detailed classification of injuries using frameworks such as the Munich Consensus Statement or the Pollock Classification, for the purpose of this article, we will focus on the broader categories of overuse and acute injuries.
a. Acute Injuries
In clinical terms, trauma is an injury resulting from the impact of an agent on a specific organism, imparting force and causing damage by subjecting the tissues to forces of tension, compression, or cutting (6).
These injuries often result from sudden, forceful events and are prevalent in high-risk environments. Examples of the most severe traumatic injuries in a tactical context include gunshot wounds and explosive-related injuries, both of which have severe consequences, both physically and psychologically, necessitating immediate attention (7). Less severe, more common, yet still significant injuries include bone fractures, muscle contusions, joint dislocations or subluxations, ligament sprains or tears, and tendon tears, among others (6).
b. Overuse Injuries
Overuse injuries result from repetitive stress and strain on specific body parts. These injuries are particularly prevalent in repetitive sports like running, as well as among tactical populations (6). Over 80% of injuries in tactical populations are overuse injuries, with a high focus on the knee and lower leg (22%), lumbar spine (20%), and ankle and foot (13%) (2). Examples include stress fractures, joint synovitis, ligament inflammation, focal muscle tissue fibrosis, tendinopathy, fasciopathy, bursitis, and others (6). We know that overuse injuries in the military environment last five times longer than acute injuries (8).
c. Tissue Healing
Regardless of the type of musculoskeletal (MSK) injury, the process of tissue healing can be summarized in three phases: the inflammatory response phase, the fibroblastic repair phase, and the maturation-remodelling phase. In Table 1, we briefly explain what happens in each phase.

2. Injury Risk
Predicting injuries has been a significant goal in much research. However, none have presented a definitive solution. While we can define the risk of injuries based on some factors—both intrinsic and extrinsic—there remains no singular solution. Intrinsic factors refer to internal characteristics or traits inherent to an individual that influence health, injury risk, and performance. On the other hand, extrinsic factors refer to external influences affecting an individual's health, injury risk, or performance, originating from outside the body (6). In Table 2, we can observe some of these factors.

Considering these factors, Sammito and his colleagues (4), proposed an injury model addressing MSk injuries in soldiers that could be adapted to other tactical populations. As illustrated in Figure 1, their proposal categorizes intrinsic and extrinsic factors as modifiable and non-modifiable and classifies them into three risk orders, with the 3rd Order representing the highest risk factor.

Meeuwisse's dynamic model of injury (presented in Figure 2) considers both intrinsic and extrinsic factors and how they interact to cause injury. In this model, intrinsic factors, related to the operator, are seen as essential but insufficient alone to cause injury. Extrinsic risk factors, on the other hand, enable injury occurrence. The combination of intrinsic and extrinsic factors makes operator vulnerable to injury, although neither alone typically causes harm. These factors prepare operators for potential injuries, with an inciting event serving as the final trigger. This event, often directly linked to injury onset, is crucial and termed the "injury mechanism." While studies usually focus on proximal factors like these events, understanding both proximal and distant factors is important (1,6).

3. Mitigating risk and enhancing injury resilience
As we see exposure to external risk factors can combine with internal factors increasing the susceptibility of the individual to injury. When intrinsic and extrinsic risk factors coincide, the likelihood of injury for the individual can be significantly higher compared to when these factors occur separately. It's crucial to recognize that both intrinsic and extrinsic risk factors are often dynamic and can change over time, and even within a single training session (6).
According to Brunkner and Khan (6), injury prevention can be characterized as being Primary, Secondary, or Tertiary:
Primary prevention: aims to prevent the occurrence of injury before it ever occurs. It focuses on addressing risk factors that can lead to injury. Primary prevention strategies include education, environmental modifications, safety regulations, and behavioural changes aimed at mitigating exposure to injury risk.
Secondary prevention: focuses on early detection and intervention to reduce the impact of injury that has already occurred. It involves efforts to identify injuries in their early stages when they are more treatable or manageable. Screening programs, regular health check-ups, and prompt medical treatment are examples of secondary prevention measures.
Tertiary prevention: aims to minimize the impact of an injury that has already occurred and to prevent complications or long-term disability. It focuses on rehabilitation, medical treatment, and supportive care to help individuals recover and regain their functional abilities. Tertiary prevention measures include physical therapy, occupational therapy, vocational rehabilitation, reconditioning and ongoing medical management to prevent recurrence or worsening of the condition.
a. Assessments and screenings
Assessments and screenings can serve as secondary prevention measures. Their main purpose is to identify vulnerabilities, primarily in intrinsic modifiable factors, and assist in the decision-making process for exercise prescription (13). Generally, tests can be classified as laboratory or field tests (14). However, in tactical settings, a different classification is often used for practicality and operational effectiveness: Generic Predictive Tests (GPTs), Task-Related Predictive Tests, and Task Simulation Tests. It is common to combine these assessments to regularly evaluate the performance of operators. When correctly applied and analysed, this combination can provide a comprehensive evaluation of motor capabilities and performance in critical occupational tasks (15,16). To evaluate intrinsic modifiable risk factors, GPTs are commonly utilized. The selection of specific tests, assessments, or screenings depends on context, budget, time limitations, and available resources. While employing a comprehensive battery of gold-standard tests would be theoretically optimal, it may be cost and time-prohibitive, and may not relate to the specific tasks and demands of the population context (2). Hence, the focus should be on identifying practical tools that provide adequate information for decision-making process. If the results of the assessment do not contribute to the decision-making process of the training prescription, then the assessment may not be the right choice. Table 3 presents some typical GPTs used in a tactical context.

b. Monitoring
If tests, assessments, and screenings are already applicable and relatively acceptable in a tactical context, monitoring, in our perspective, is still not well established. This may be one of the main reasons for the prevalence of overuse injuries in tactical settings.
Like in sports, tactical workload monitoring has been broadly discussed recently, mainly due to technological advancements and increased concern about injury and illness prevention, particularly given the risk of deadly incidents (17–20). The main challenges are not only the practicability and reliability of using these instruments and algorithms, but also the sociocultural biases and the interpretation of data in the field, especially in the absence of a sports scientist or sports medicine professional.
Monitoring continues to serve as both primary and secondary prevention measures and is a valuable tool for evaluating modifiable external factors and understanding the implications of non-modifiable external factors on operators. Gabbett and colleagues (21), suggest a monitoring cycle that can be tailored to suit the needs of tactical environments. This cycle follows a systematic approach to interpret athlete monitoring data, starting from the exposure to a single external training stimulus, through to the subsequent exposure. When each step of the cycle is integrated with the preceding ones, it offers understanding on interpreting the data and recommending interventions to support appropriate training adjustments. To aid practitioners in decision-making processes, they have created a matrix for each step of the cycle.

c. Injury resilience
As we have already seen, over 80% of injuries in tactical populations are overuse injuries, with a high incidence in the lower limb and lumbar spine. The data on overuse injuries in tactical populations provides essential guidelines for enhancing the resilience and performance of operators (2). To address these issues, several key strategies can be implemented.
Firstly, a properly designed and executed warm-up can help prevent injuries and can be combined with specific injury prevention programs, particularly during training sessions. For these programs to be effective in reducing injuries and enhancing performance, it is crucial to consider the specificity of the activity, the environment, the duration and intensity of the warm-up, as well as ensuring participants follow them diligently. Additionally, it is important for operators to understand the purpose of the warm-up and the benefits they can expect from it (2,9,22–26).
In addition, a slower progression in running volume is recommended. The guideline for workload suggests no more than a 10% increase per week. Reducing running volume is another critical component of injury prevention. While running is a fundamental aspect of many tactical training programs, excessive mileage can contribute to overuse injuries, particularly in the lower extremities. By incorporating alternative cardiovascular exercises, operators can maintain their aerobic fitness while giving their joints and muscles a necessary respite from repetitive impact (2,6,9).
Increasing the variability of exercises within training programs is essential for operators’ resilience. A diverse exercise regimen that includes mobility, proprioceptive, multiaxial, and neuromuscular exercises enhance overall physical resilience. Mobility exercises improve joint range of motion and flexibility, which are vital for functional movement and injury prevention. Proprioceptive exercises, focusing on balance and body awareness, help improve coordination and reduce the risk of falls and related injuries. Multiaxial exercises involve movements in multiple planes of motion, promoting functional strength and stability across various muscle groups. These exercises mimic real-life movements and challenges that operators might encounter in the field, preparing them better for operational demands. Neuromuscular exercises emphasize the connection between the nervous and muscular systems, improving reaction time, agility, and overall motor control. Incorporating these types of exercises ensures a well-rounded training program that addresses all aspects of physical fitness and injury resilience (2,9,22–26).
Education and awareness are also crucial components of injury prevention. Operators should be educated about the importance of recognizing early symptoms of overuse injuries and seeking prompt medical attention when needed. Emphasizing the significance of proper warm-up and cool-down routines, adequate exercise technique, hydration, and nutrition can further enhance recovery and resilience (2).
Despite these guidelines, by evaluating intrinsic and extrinsic factors and identifying injury risks, we can implement injury resilience and prehabilitation programs more efficiently. This approach focuses on individually modifiable factors, particularly identified weaknesses, imbalances, and vulnerabilities, and can be more effective than simply following the guidelines.
4. Injury prevention models and rehabilitation
It is essential to recognize that everyone faces a certain potential risk of injury during their sporting, exercise, or occupational activities. Furthermore, every sport, exercise, or occupation carries a level of risk for its participants or professionals. It is unrealistic to expect zero risk, particularly in a tactical context. With this understanding, our focus shifts to preventing injuries and mitigating these risks and making operators more injury-resilient. To do so effectively, we must first identify the sources of risk (2).
a. Injury prevention models
In 1992, Van Mechelen (10) proposed a four-step sequence of prevention that remains relevant today. In summary, this four-step sequence is based on the following line of thinking:
Step A: Understanding the scope and scale of the injury problem. It includes collecting data on the incidence, severity, and types of injuries occurring within a specific population or sport.
Actions: Conduct epidemiological studies; Analyse injury patterns (identify most common and severe injuries); Gather data on the context in which injuries occur.

Step B: Identifying the causes and mechanisms behind the injuries. Understanding why and how injuries happen is crucial for developing effective prevention strategies.
Actions: Investigate intrinsic and extrinsic factors contributing to injuries; Study the biomechanics and physiological aspects of the activity (specific injury mechanisms).
Step C: Based on the insights gained from the first two steps, this step involves developing and implementing strategies to prevent injuries.
Actions: Design interventions (training programs, protective equipment, educational campaigns, etc); Develop conditioning and rehabilitation programs to address identified risk factors; Implement strategies and monitor their application in real-world settings.
Step D: The final step assesses the impact of the implemented preventive measures to determine their effectiveness.
Actions: Conduct follow-up studies to compare injury rates before and after the implementation of preventive measures; Analyse data to see if the measures have led to a significant reduction in injuries; Adjust and refine preventive strategies based on feedback and new insights.
Years later, Caroline Finch presented a revision of this sequence named Translating Research into Injury Prevention Practice (TRIPP). While Van Mechelen's model provides a strong foundation for injury prevention research, Caroline Finch's TRIPP model extends this framework by emphasizing the importance of understanding and evaluating the practical application of preventive measures (8,11).
Stage 5: Understanding the practical context in which the preventive measures will be applied. It involves identifying barriers and facilitators to the implementation of injury prevention strategies in real-world settings.

Actions: Assess the environment, resources, and stakeholders involved in the implementation; Identify potential challenges and enablers within the specific context (e.g., cultural, organizational, logistical); Engage with practitioners, coaches, and athletes to understand their perspectives and needs.
Stage 6: Evaluating how well the preventive measures are being implemented in practice. It focuses on process evaluation to ensure that the strategies are applied as intended and to identify areas for improvement.
Actions: Monitor the fidelity of implementation, adherence to protocols, and the reach of the intervention; Collect qualitative and quantitative data on the implementation process; Identify and address any deviations, barriers, or issues encountered during implementation.
While the models discussed are specifically designed for sports athletes, they also form the basis for some models used with tactical populations. One widely recognized example is the Human Performance Optimization (HPO) model. This model provides a detailed, evidence-based approach to optimizing performance and preventing injuries (12).
Step 1: Injury surveillance: Identifies the scope and magnitude of the problem.
Actions: Collect data on injury rates, types, and patterns within the population of interest; Analyse injury data to identify trends, risk factors, and high-risk activities or tasks.
Step 2: Task and demand analysis: Data collection in the field— observing the tasks that performed as part of tactical training, physical training, and employment/missions.
Actions: Evaluate the physiological, biomechanical, physical, and cognitive demands of the tasks performed by individuals or teams; Identify factors contributing to task-related injuries or performance limitations.

Step 3: Predictors of injury and optimal performance: Determination of characteristics that predict injury and performance—providing a target for physical training and interventions.
Actions: Determine intrinsic and extrinsic factors contributing to injuries and influence performance on your context; Conduct assessments and screenings to identify strengths, weaknesses, and areas for improvement (take care of specificity of the job task).
Step 4: Design and validation of interventions: The design of any intervention for injury prevention or performance optimization must focus on the target populations injury profile, their occupational demands, and the identified predictors of injury and performance.
Actions: Consider space requirements, austere environments, and available equipment when designing interventions; Focus on validating the effectiveness of the program to modify predictors of injury and performance identified in the previous step; Ensure that interventions are tailored to accommodate the unique challenges and constraints of tactical environments; Prioritize interventions that address specific risk factors and enhance performance outcomes within the tactical population; Emphasize the importance of validation and effectiveness testing to ensure that interventions are suitable for implementation in real-world settings.
Step 5: Program integration and implementation: Determination of the logistics and actions necessary for successful delivery of the intervention.
Actions: Integrate interventions into existing training and operational protocols; Develop protocols and guidelines for implementing interventions consistently across the organization.
Step 6: Monitor and determine the effectiveness of the program: conduct long term tracking of injuries and performance as the HPO program is exposed to the larger target population.
Actions: Establish monitoring systems to track the implementation of interventions and their impact on injury rates and performance outcomes; Evaluate the effectiveness of the program through ongoing data analysis and feedback mechanisms; Adjust interventions and protocols based on monitoring results to optimize program effectiveness.
b. Injury rehabilitation and return to duty
Rehabilitation is a form of tertiary prevention, and it involves a process that passes through multiple phases. Depending on the injury, it could be a painfully long process or a relatively short, pain-free one. However, it is crucial for the operator to understand that there are no shortcuts. Skipping or rushing through any of the phases increases the risk of re-injury or long-term issues. Figure 7 presents the typical phases of the rehabilitation process.

A rehabilitation program, ideally and theoretically, should benefit from various inputs. This includes contributions from medical and surgical specialists, sports physicians, physiotherapists, exercise physiologists, rehab trainers, and strength and conditioning (S&C) coaches. The success of the rehabilitation and reconditioning process significantly relies on the integrated and effective collaboration of these experts, with mutual respect for each other’s professional abilities, along with the operator's own insights and emotions (25). In the sports context, this interdisciplinary approach is well-established, with almost all sports teams having their own sports medicine team. However, in the tactical context, this is not always the case.
There are two typical models of rehabilitation. In one the medical team might retain control of the athlete's care for too long without involving the S&C coaches, who need to be aware of the healing stages of the injured tissue. Equally problematic is a scenario where technical coaches (Tactical Fitness Instructors team) are not involved until late in the rehabilitation process, missing opportunities for low-load technical training (25). This model is presented in the Figure 8 and its normally called as poor model in sports context that we adapted.

A much better approach involves S&C coaches collaborating closely with physiotherapists from the early stages of rehabilitation, and technical coaches being involved throughout the process. This ensures the operator can prepare for performance while simultaneously recovering from the initial injury (25). This model is presented in the Figure 9 and its normally called as well-integrated model in sports context that we adapted.
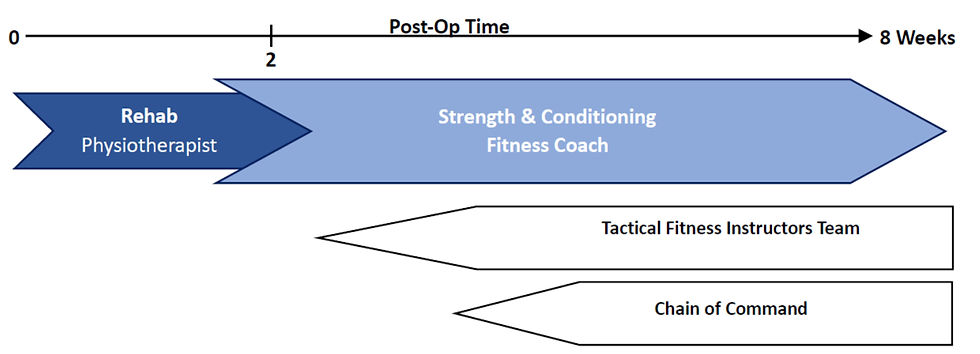
Figure 10 shows a detailed, step-by-step outline of a rehabilitation process. It's important that each rehabilitation program is tailored to the individual, using criteria-based progression to ensure safe movement through different phases and to lower the risk of re-injury. Various objective criteria can be used throughout the rehabilitation stages, such as grading effusion, assessing muscle soreness, monitoring running progression, evaluating context-specific agility, and performing functional tests. Reconditioning is a vital part of this stepwise rehabilitation program, ensuring that the injured operator is fully prepared to return to duty (27).

Communication is key during this process. When the operator has been treated by a physician, physiotherapist, and S&C coach from different institutions, this communication can be very fragile or non-existent, often leading to a poor or incomplete rehabilitation process and increasing the risk of re-injury and long-term issues (2,9,25). In such cases, it is vital for the operator to understand the importance of this communication and to request reports, indications, and contraindications from each professional to share with the others. Ideally, despite institutional barriers and personal biases, these professionals should communicate directly with each other about each case. However, this is often very complex to achieve, so providing reports is a practical and functional solution in such situations (9).

References
I really like the article, but it is a little too theoretical. I would love to see some return-to-duty protocols.
From what I've seen, getting back to work is often a bit muddled and not given enough attention, which can cause folks to get hurt again and be off even longer. The article's great; it's a solid read that all tactical personnel should check out.😁